Medscape article on the treatment of Meniere disease #archive
Posted By RichC on March 27, 2019
A couple of decades ago I suffered from Ménière disease (Ménière’s disease) and struggled to find treatment and relief from the miserably vertigo episodes. One does not understand how debilitating and miserable that this be, so much so that any potential treatment, regardless of the risk, seemed worth it at the time. In my case, I opted for the endolymphatic sac decompression or shunt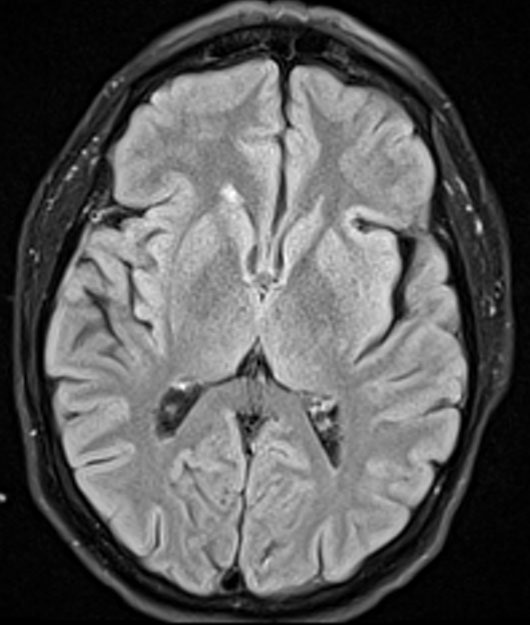 placement surgical treatment since it was what my ENT who specialized in Ménières was doing here in Cincinnati … and I was a good candidate (young/healthy). I had already had all the tests, scans, etc and worked for over a year with sodium diet control, OTC products, diuretics and diazepam with little to show for it. Thankfully for me (although knowing what is known now is questionable) the surgery was successful and within a month or so it improved my life immensely (fewer and lessening in intensity). The hearing in my right ear was gone, but I have retained hearing and balance for the most part from my left ear. Except for the tinnitus and an odd relapse that was treated at the Cleveland Clinic a decade later with a tympanic steroid injection I’ve been vertigo free … but the “drop attacks” disappeared. Thank God!
placement surgical treatment since it was what my ENT who specialized in Ménières was doing here in Cincinnati … and I was a good candidate (young/healthy). I had already had all the tests, scans, etc and worked for over a year with sodium diet control, OTC products, diuretics and diazepam with little to show for it. Thankfully for me (although knowing what is known now is questionable) the surgery was successful and within a month or so it improved my life immensely (fewer and lessening in intensity). The hearing in my right ear was gone, but I have retained hearing and balance for the most part from my left ear. Except for the tinnitus and an odd relapse that was treated at the Cleveland Clinic a decade later with a tympanic steroid injection I’ve been vertigo free … but the “drop attacks” disappeared. Thank God!
The surgery I had after after little success from diet and medications is the same that astronaut Alan Shepard had in the 1960s.  His success and return to flight status (eventually flying an Apollo space capsule on top of a Saturn V rocket to the moon!) was of great inspiration to me as at the time I was actively involved in flying and building experimental airplanes. Knowing what is now available, I’m sure I would have gone the ranstympanic medication perfusion route before ever moving forward with the destructive and far riskier surgery (Van Gogh’s Starry Night art above – previous post).
His success and return to flight status (eventually flying an Apollo space capsule on top of a Saturn V rocket to the moon!) was of great inspiration to me as at the time I was actively involved in flying and building experimental airplanes. Knowing what is now available, I’m sure I would have gone the ranstympanic medication perfusion route before ever moving forward with the destructive and far riskier surgery (Van Gogh’s Starry Night art above – previous post).
The point of this post is to archive a great write-up/update of the Surgical Treatment of Ménière Disease by John C Li, MD published in Medscape (a great resource) and if I ever need to find this information again for anyone else who may be suffering. This is by far the best information I’ve ever read – and believe me, I’ve read a lot on the subject.
Surgical Treatment of Meniere Disease
Overview
Background
The term endolymphatic hydrops refers to a condition of increased hydraulic pressure within the inner ear endolymphatic system. It is often used synonymously with the terms Ménière disease and Ménière syndrome. [1] However, Ménière disease is more correctly understood as endolymphatic hydrops without a determined etiology—that is, idiopathic endolymphatic hydrops—whereas Ménière syndrome can occur secondary to various processes interfering with normal production or resorption of endolymph.Excess pressure accumulation in the endolymph can cause a tetrad of symptoms: (1) fluctuating hearing loss, (2) occasional episodic vertigo (usually a spinning sensation, sometimes violent), (3) tinnitus or ringing in the ears (usually low-tone roaring), and (4) aural fullness (eg, pressure, discomfort, fullness sensation in the ears).
Although the disease itself is not lethal, significant morbidity can arise from various manifestations of the disease. Vertigo can cause devastating accidents and falls. Hearing loss is often progressive over time. Many patients are unable to work and are forced to claim disability.
Surgical management of Ménière disease is reserved for cases in which medical treatment fails. The future of Ménière treatment lies in the use of methods that are less invasive and less destructive than current ones to control vertigo. The concept of transtympanic delivery of medications is appealing. As new medications and delivery systems are discovered, more refined approaches to a cure may evolve.
Go to Meniere Disease (Idiopathic Endolymphatic Hydrops) for complete information on this topic.
Indications
Surgery is indicated for Ménière disease that is refractory to medical management. Typically, failure to respond to 3-6 months of medical therapy is an indication for surgery. However, patients with severe debility may undergo surgery sooner. Any underlying medical causes of Ménière syndrome should be treated before surgical therapy is undertaken. The diseased ear must be clearly identified.Contraindications
Patients should be in good health and able to withstand surgery and anesthesia. Obtain a thorough history and perform a careful physical examination before the procedure to detect any medical contraindications. Surgery is not necessarily contraindicated in elderly patients. Patients in their 80s have tolerated labyrinthectomy fairly well.Otitis media and mastoiditis are contraindications for surgery. Resolve these infections before proceeding to avoid an increased risk of meningitis.
Bilateral vestibular disease is a relative contraindication for destructive procedures because of the risk of complete loss of inner ear function (ie, Dandy syndrome). Hypersensitivity or allergy to the target medication is a contraindication for aminoglycoside perfusion.
One principle of ear surgery is to avoid operating on an ear that provides all of the patient’s hearing because of the risk of creating profound bilateral deafness. This rule applies to most otologic surgical procedures.
Relevant Anatomy
The peripheral vestibular system is an integral part of the labyrinth that lies in the otic capsule in the petrous portion of the temporal bone.The vestibular system, which is the system of balance, consists of 5 distinct end organs: 3 semicircular canals that are sensitive to angular accelerations (head rotations) and 2 otolith organs that are sensitive to linear (or straight-line) accelerations.
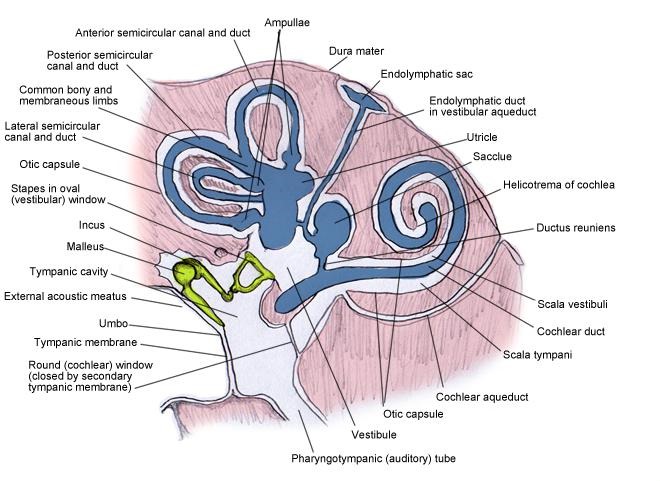
The labyrinthine cavity is essentially formed of the membranous labyrinth encased in the bony osseus labyrinth (see the image below). The osseus labyrinth is a series of bony cavities within the petrous temporal bone; the membranous labyrinth is the communicating membranous sacs and ducts housed within the osseus labyrinth. The membranous labyrinth is cushioned by the surrounding perilymph and contains the endolymph within its confines. The membranous labyrinth also has cochlear, vestibular, and semicircular components.
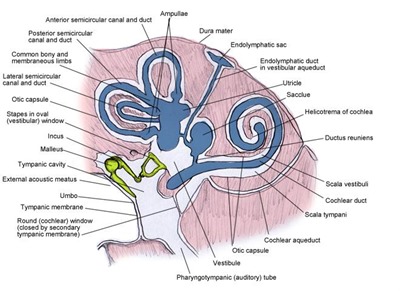
Inner ear: bony and membranous labyrinths.
For more information about the relevant anatomy, see Vestibular System Anatomy, Inner Ear Anatomy, Ear Anatomy, and Skull Base Anatomy.Preparation
Preoperative Evaluation
Surgeons must definitively decide which ear is affected and rule out other medical causes of Ménière syndrome before proceeding to surgery. Appropriate laboratory tests are done to identify other problems. Surgery should proceed only after these results rule out relevant comorbidities.Magnetic resonance imaging (MRI) is helpful to rule out acoustic neuroma as the source of vertigo. Electrocochleography (ECOG) can help in localizing the problematic ear. Electronystagmography (ENG) can be helpful to demonstrate reduced vestibular responses and is essential to establish vestibular function in the nonsurgical ear when a destructive procedure is contemplated.
Document inner ear function preoperatively. Because hearing fluctuates, several preoperative audiograms may be required to capture the range of hearing function. Audiograms can help in identifying the diseased side.
Preoperative Counseling
After destructive procedures, patients may initially feel worse than ever. Accordingly, substantial preoperative counseling is required to prepare patients adequately for the possible sequelae. Postoperative counseling will be indicated as well.Technique
Overview
Surgical management of Ménière disease is reserved for cases in which medical treatment fails. Typically, failure of a 3- to 6-month trial of diuretics and dietary control justifies a more aggressive approach. Patient factors (eg, severity, occupation, degree of disability, individual tolerance) also affect the timing of surgery.Surgical therapy has significantly evolved over the past 30 years. Beyond the general agreement that surgical therapy for Ménière disease is reserved for medical treatment failures, considerable controversy exists. Historically, multitudes of clever surgical procedures have been invented, tested, and discarded. Those currently in use may be divided into 2 major categories: destructive and nondestructive.
The rationale for using destructive procedures to control vertigo is as follows: Endolymphatic hydrops causes fluid pressure to build up in the inner ear, causing temporary malfunction and misfiring of the inner ear. Abnormal signals traveling to the brain cause vertigo. Therefore, destruction of the inner ear or nerve prevents abnormal signals from reaching the brain. The brain eventually compensates for the loss of the damaged labyrinth, provided that the other inner ear is working properly.
Destructive procedures have several problems. The decision to destroy the function of a misfiring inner ear is predicated on adequate function of the opposite ear. However, Ménière disease can be bilateral in 7-50% of patients. Therefore, the author recommends avoidance of destructive procedures in patients with bilateral Ménière disease. Because balance and hearing are closely intertwined in the labyrinth, destruction of the balance portion poses a high risk of destroying hearing as well. Destructive procedures are irreversible and are reserved for severe cases.
Nondestructive procedures are aimed at improving the state of the inner ear. Nondestructive procedures are less invasive than destructive ones and do not preclude use of other treatment modalities.
This article covers the 4 most generally accepted management options: endolymphatic sac decompression or shunt placement, transtympanic medication perfusion, vestibular nerve sectioning, and labyrinthectomy.
Endolymphatic Sac Decompression or Shunt Placement
In theory, the endolymphatic sac procedure decreases the buildup of endolymphatic pressure by removing petrous bone that encases the endolymph reservoir. [2, 3, 4] This allows the reservoir sac to expand more freely than before and allows the pressure to dissipate. In addition, some surgeons insert a drain or valve from the endolymphatic space to the mastoid or subarachnoid space to reduce pressure further.Exposure of the endolymphatic sac is essentially extended mastoidectomy. Special care is taken to skeletonize the sigmoid sinus, posterior fossa dura, and posterior semicircular canal. Thin egg-shelled bone is removed from the posterior fossa dura and sigmoid sinus. The endolymphatic sac is distinguished from the dura by characteristic differences its color and texture (ie, the sac is thicker and whiter than surrounding tissue).
The location of the sac can vary somewhat, but it is generally immediately posterior or posteroinferior to the posterior semicircular canal. In endolymphatic sac decompression, the procedure is terminated when all of the bone overlying the sac is removed. Shunt procedures involve incising the lateral leaf of the sac and inserting a drainage tube into the internal lumen of the endolymphatic duct. Shunts can drain into the subarachnoid space or the mastoid space.
Success rates of 60-90% have been reported for vertigo control and stabilizing hearing acuity. Success rates for endolymphatic sac decompression and for shunt procedures do not seem to differ substantially.
Morbidity and mortality risks endolymphatic sac decompression are relatively low. The risk of hearing loss and facial nerve damage is minimal when the procedure is done by experienced surgeons. One study showed that one of the complications of this procedure was a low frequency conductive hearing loss. Although it could be related to bone chips and scarring, the authors postulated that another possibility might be that the opening of a third window within the system creates a slight air bone gap. This possibility is something to be aware of while performing endolymphatic sac decompression. [5]
The endolymphatic sac procedure is perhaps one of the most controversial issues in neuro-otology. [6, 7, 8, 9] Critics state that the procedure is completely worthless. Authors of the famous Danish study argue that endolymphatic surgery is as useless as sham surgery and that any benefit is a placebo effect. [10]
Proponents of sac surgery argue that patients really do improve. Compared with destructive procedures, endolymphatic sac procedures have low risk and morbidity and can provide relief to patients in whom medical therapy fails. [11]
Transtympanic Medication Perfusion
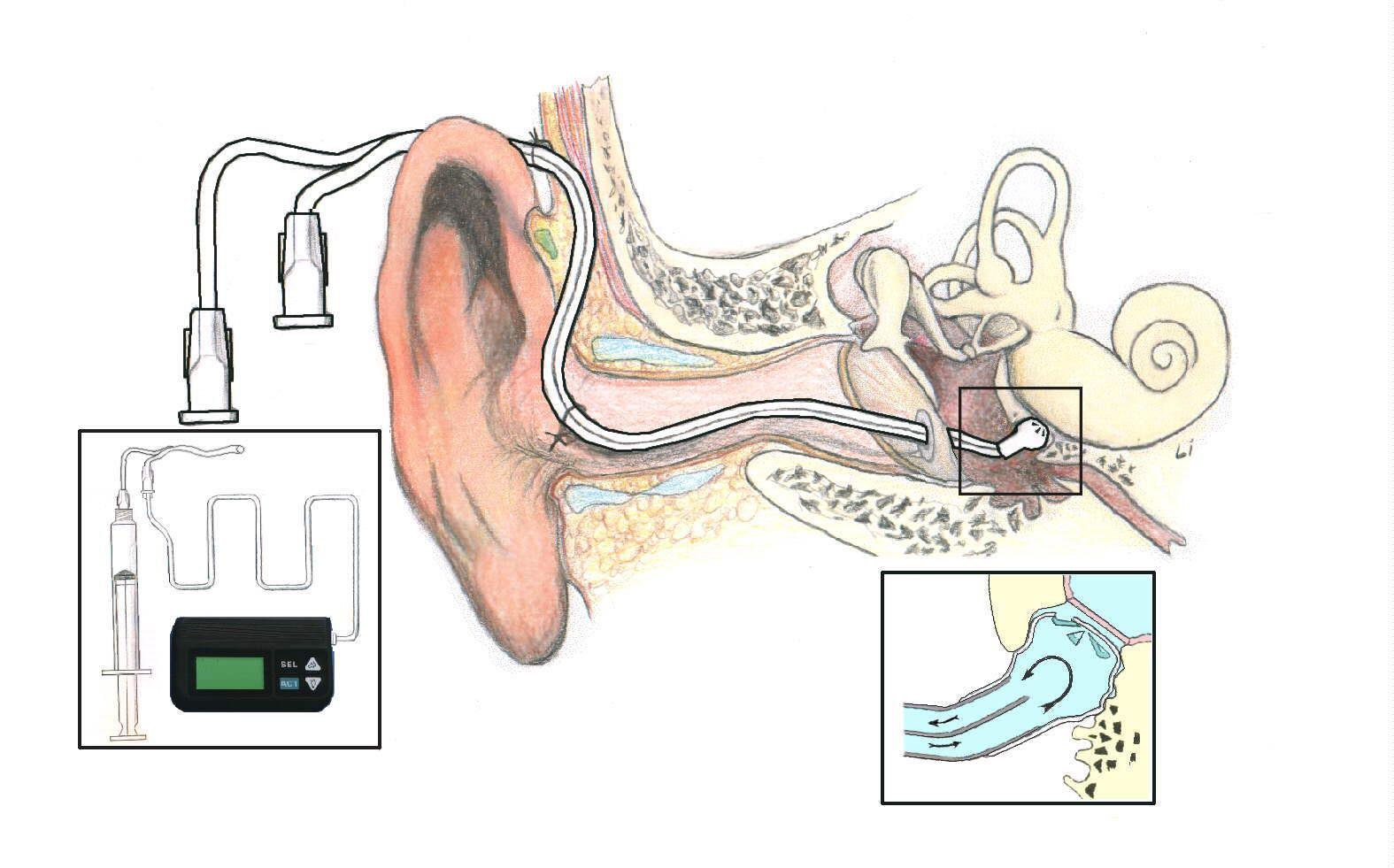
Transtympanic medication perfusion is becoming an established treatment modality. Popularized by Dr John Shea in 1995, the procedure is still evolving. Although the techniques, insertion devices, indications, and pharmacologic compositions vary, the basic concept remains the same.In this procedure, medications that may exert some effect on Ménière disease are delivered to the middle ear cavity through a myringotomy. From there, medication is absorbed into the inner ear, presumably through the round window membrane (see the image below). This method facilitates the application of high concentrations of medication with minimal systemic effects.
The Round Window Microcatheter was one of the first transtympanic instillation devices used to administer drugs to the inner ear. It is no longer available and has been supplanted by simpler transtympanic injection methods using a needle through the drum, drops through a tube, or drops into a Silverstein Microwick.
Transtympanic medication perfusion is relatively low risk and simple to perform. It is essentially similar to the placement of tympanostomy tubes, which can be done in an office or outpatient setting. Innovations such as the round window microcatheter and Silverstein MicroWick were designed to channel medication flow directly to the round window niche. Theoretically, this method reduces dosing inconsistencies due to loss of medication down the eustachian tube. The round window microcatheter has lost favor and is no longer being produced.
When steroids are used, transtympanic perfusion is considered a nondestructive procedure. Transtympanic steroid application is useful, particularly when patients have poor tolerance for the systemic adverse effects of steroids. Furthermore, high concentrations can be administered by using this approach. Although results of long-term studies are not yet available, success rates appear to be favorable.
When aminoglycosides are used, transtympanic perfusion is considered a destructive procedure. The effects of transtympanically administered aminoglycosides are concentrated in the affected ear rather than in both ears. Streptomycin [12] is difficult to obtain in the United States because of restrictions imposed by the US Food and Drug Administration (FDA); therefore, gentamicin [13] is more widely used. Early studies show an efficacy of about 90%. Some authors report substantial worsening of hearing in 5-25% of patients.
Vestibular Nerve Sectioning
Sectioning the diseased balance nerve can be the ultimate solution for patients with useful hearing in the affected ear. Although hearing and balance functions are housed in 1 common chamber within the inner ear, their neural connections to the brain separate themselves into distinct nerve bundles as they course through the internal auditory canal. This anatomic separation facilitates the isolation and ablation of balance function without disturbing hearing function.Vestibular nerve sectioning is similar to approaches used for acoustic neuroma, in that it involves the opening of the internal auditory canal. Vestibular nerve sections are typically performed through either a retrosigmoid or a middle-fossa approach. The translabyrinthine approach would not spare hearing and is used only as added insurance when labyrinthectomy is intended.
Surgeons generally agree that the retrosigmoid approach is less technically difficult than the middle-fossa approach. The retrosigmoid approach proceeds through a small craniotomy posterior to the sigmoid sinus. Exposure of the cerebellopontine angle allows visualization of the eighth cranial nerve.
Proper identification of the vestibular nerve through observance of proper anatomic relationships is mandatory to avoid severing facial and cochlear nerves. Because the nerve bundle rotates as it exits the internal auditory canal, the vestibular nerve moves from its lateral position to a more superior location. The vestibular nerves are those closest to the tentorium. Monitoring of the facial and cochlear nerves by means of intraoperative auditory brainstem response (ABR) monitoring is helpful.
The middle-fossa approach to vestibular nerve sectioning involves creating a 5 × 5-cm craniotomy in the middle fossa just superior to the temporal line above the external ear canal. The dura of the middle fossa is retracted superiorly to expose the bone. After the proper anatomic landmarks are identified, the internal auditory canal is identified and opened, and the vestibular nerve is sectioned as laterally as possible. Fat is packed into the internal auditory canal and held in position by the temporal lobe dura. The craniotomy is then closed to terminate the procedure.
The middle fossa approach achieves slightly more complete ablation of vestibular function. Because the vestibular fibers are cut immediately as they exit the vestibular end organ, stray vestibular fibers have little opportunity to cross over and travel along the facial and cochlear nerves. In the retrosigmoid approach, the vestibular nerve is sectioned much more medially, possibly after stray vestibular fibers have crossed. Although unusual, failure of the retrosigmoid approach may be attributed to these crossed fibers.
Difficulty in locating the internal canal and limited exposure in the canal because of the position of the facial nerve are disadvantages of using the middle-fossa approach. Cutting the vestibular nerve without exerting pressure on cochlear and facial nerves is difficult because the vestibular bundle lies deep within the canal. Furthermore, the risk of damaging the cochlear artery, which causes hearing loss, is higher with the middle-fossa approach than with the retrosigmoid approach.
Advantages of vestibular nerve sectioning are a vertigo-control rate of about 95-98% and an approximately 95% success rate in preserving hearing preservation in the surgically treated ear. The risks of the procedure are those inherent to craniotomy and acoustic neuroma surgery. Facial-nerve damage, hearing loss, exacerbation of tinnitus and dizziness, cerebrospinal fluid (CSF) leakage, headaches, hemorrhage, and infection (meningitis) are possible but rarely develop.
After surgery, patients generally require 3-5 days of inpatient care. Adaptation to the surgical loss of 1 vestibular apparatus usually takes weeks to months. Vestibular rehabilitation during this period is often helpful.
Labyrinthectomy
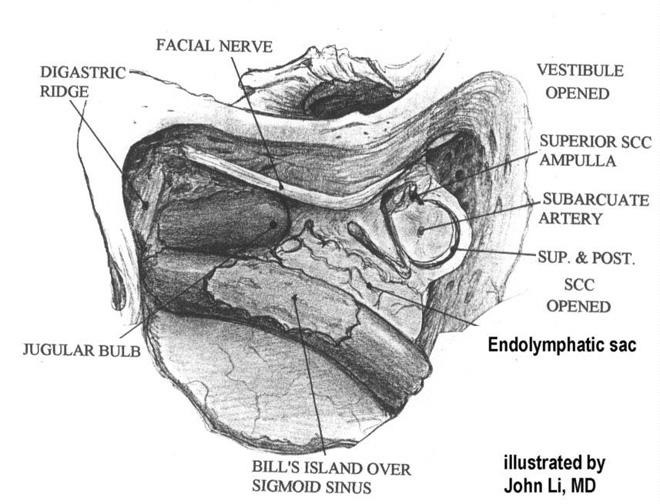
Labyrinthectomy has the advantage of a high cure rate (>95%) and is useful in patients in whom Ménière disease has destroyed their hearing on the affected side. [14] Labyrinthectomy involves ablation of the diseased inner-ear organs but does not require entry into the cranial cavity; thus, it is less complex than vestibular nerve sectioning (see the image below).
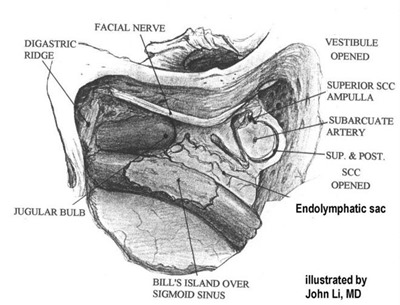
Intraoperative view of left ear treated with labyrinthectomy; endolymphatic sac can be seen in this view.Labyrinthectomy can be performed via either a transcanal approach or a basic mastoidectomy approach. The transcanal approach proceeds through the external ear canal. First, a tympanomeatal flap is elevated. Next, a right-angle pick is inserted through the oval window and maneuvered so as to disrupt and scramble the nerve tissues of the labyrinth. Sometimes, a drill is used to connect the round and oval windows to improve exposure to the neuroepithelium.
The basic mastoidectomy approach involves extending the mastoidectomy by drilling through the semicircular canals. This allows more complete ablation of the labyrinthine neuroepithelium than can be achieved with the transcanal approach.
Labyrinthectomy is a bit less invasive than vestibular nerve sectioning. Craniotomy is not required; therefore, the risk of CSF leakage and meningitis is reduced. Patients typically require a few days of inpatient care. Adaptation to the surgical loss of 1 vestibular apparatus usually takes weeks to months. Vestibular rehabilitation during this period is also helpful.
Post-Procedure
Postoperative Care
Postoperative care is different for each type of surgical procedure performed. Patients undergoing destructive surgery can expect severe vertigo and imbalance for the first few days. Liberally dispense medications to alleviate nausea and vomiting during this time. Early vestibular rehabilitation is helpful in achieving rapid compensation for loss of unilateral vestibular input.Expected Outcomes
The prognosis of patients with surgically treated Ménière disease varies with the treatment. Endolymphatic sac surgery controls vertigo in 60-90% of patients, it has a low risk of hearing loss, and it can improve the patient’s hearing over time.Destructive surgeries (eg, labyrinthectomy, vestibular nerve sectioning) have success rates of about 95-98%. However, destructive surgeries have a greater risk of hearing impairment.
Transtympanic injection of medications is a relatively new surgical approach and thus is still being evaluated. Success rates near 90% have been reported.
Complications
Many potential risks and complications exist, but they develop relatively rarely. As with any ear surgery, hearing loss, tinnitus, dizziness, facial paralysis, hematoma, bleeding, cerebrospinal fluid (CSF) leakage, taste disturbance, and mouth dryness are possible.Of the surgical treatments discussed in this article, transtympanic injections are the least risky. Overall, transtympanic injections are equivalent to tympanostomy tube placement in terms of risk. Specifically, risks vary somewhat according to the type of medication applied. Steroids have been fairly safe when given transtympanically. Aminoglycosides can adversely affect hearing. Hearing loss statistics range from 5-25%. Some authors have noted otitis media, otorrhea, and prolonged perforations.
Endolymphatic sac decompression incurs the same risks as standard mastoidectomy does. Endolymphatic sac shunts can increase the risk of CSF complications (eg, leakage, meningitis) when they penetrate the subarachnoid space.
Vestibular nerve sectioning involves craniotomy and therefore carries the highest risk of CSF complications and increases the risk of damage to the facial and cochlear nerves compared with standard mastoidectomy.
Other complications depend on the approach used. The retrosigmoid approach is associated with a high incidence of traction headache, which has been attributed to postoperative adhesion of the scalp to the dura, particularly when the bone window is not replaced. Violation of the tracts of the labyrinthine air cells can also be a pathway for CSF leakage if these openings are not covered with bone wax.
Long-Term Monitoring
In general, outpatient follow-up requires substantial supportive care. Patients are often dizzy and report feeling worse than ever before. Outpatient vestibular rehabilitation has been helpful in patients undergoing destructive procedures.Patients who have undergone endolymphatic sac decompression notice conductive hearing loss as a consequence of postoperative accumulation of blood behind the eardrum. Some patients have dizziness immediately after surgery.
Long-term follow-up can be scheduled for every 3-6 months initially and then changed to an as-needed schedule.
Comments