The Dow moves above 13,000, but closes 0.1% down instead
Posted By RichC on February 27, 2012
The Dow once again inches past the 13,000 market, but somehow can’t quite close above this psychological level.
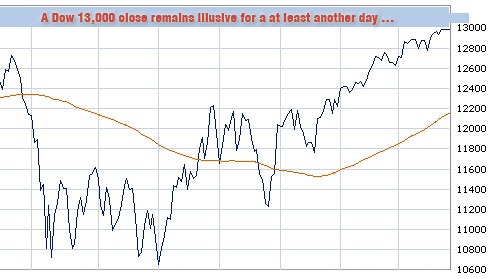
For a few moments Monday, it looked like it was finally happening. But the Dow Jones Industrial Average failed yet again to close above 13000.
The average ended down 1.44 points, or less than 0.1%, at 12981.51. It was the fifth day traders had toyed with the 13000 marker, a level seen as psychologically, if not technically, important to the market.
Gas prices, car rentals and the economy of traveling by car
Posted By RichC on February 26, 2012

Katelyn and Taylor back in 1991 preparing for a road trip
While planning a couple upcoming trips after the recent jump in gasoline prices (over $3.50 and rising), I reflected on the “good ol’ days” when we would hop in the Oldsmobile Custom Cruiser station wagon and take off on long trips at what seemed like a moments notice. I’m sure we did a little more planning that that, but I don’t recall fretting about how much fuel would cost us. Nowadays, even with improved fuel efficiency, most young families have to think twice before buzzing over the river and through the woods.
I’ve reduced my sales call visits to customers and have been rethinking both my business travel and personal trips this past year. In fact, last week I even tweaked my “cost to drive” spreadsheet which now easily justifies renting a fuel efficient car for a couple longer upcoming trips. It just doesn’t make sense to drive my <20 mpg Pilot IF I can rent a 35-40 mpg car (with unlimited miles) and can keep the miles off my Honda – I didn’t even factor in mileage depreciation, oil changes or tires. Something to think about if you are planning a longish road trip. (below is the 2000 road trip comparison)

Who designs KitchenAid appliances – engineers or accountants?
Posted By RichC on February 25, 2012
 While cleaning out our KitchenAid refrigerator and freezer on Saturday, I wondered “what were the design engineers thinking” when they used corrosive fittings?
While cleaning out our KitchenAid refrigerator and freezer on Saturday, I wondered “what were the design engineers thinking” when they used corrosive fittings?
For all the years companies have been designing and building ice makers which operate in moisture prone environments, one would think someone might have suggested spending a few more pennies on stainless steel or even nylon fittings. I don’t think the rust has affected the taste of of the ice or caused any harm, but I can’t say the design flaw has me recommending KitchenAid appliances. Then again, the same can be said for the grade of stainless steel in our newish Bosch dishwasher (a little rust is appearing on the door edges — grr).
Archiving sailboat bottom paint information for Encore
Posted By RichC on February 25, 2012
Ahh … love that full flavored and steaming cup of coffee on a Saturday morning.

While sifting through my pile of magazines and deciding what to toss and what to keep, I’ve clipped a few items I want to keep … but am just not sure how to archive them? Sometimes I still toss stuff in a folder and put in the file drawer, other times I scan and save to a hard drive, CD or upload to the computer and often I just scribble notes in my Moleskine notebook. I really do lack an organizational system that works.
ARCHIVED BELOW
I doubt the bottom paint charts or text included at the bottom will be of interest to those outside the boating world, but perhaps the mini test below will help someone on the next crossword puzzle (You’ll have 60 seconds to review the “parts of a sail” before the answers appear).

Click for full article from Practical Sailor’s upcoming March 2012 issue (although it might require a full subscription?)

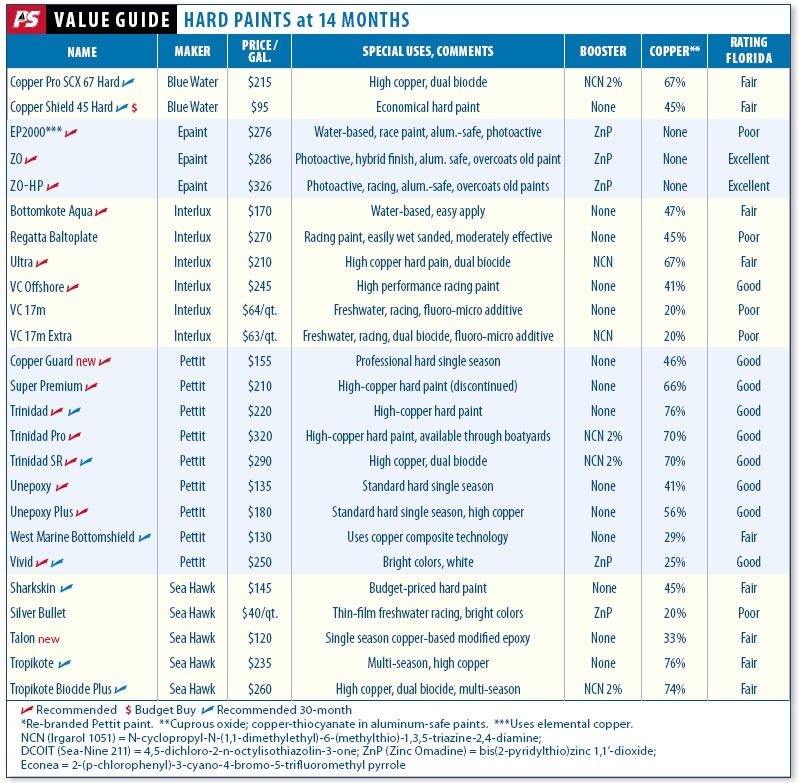
Since I’ll eventually be repainting the bottom of Encore, I figured it might be a good idea to starting thinking about the cost.
Conclusion
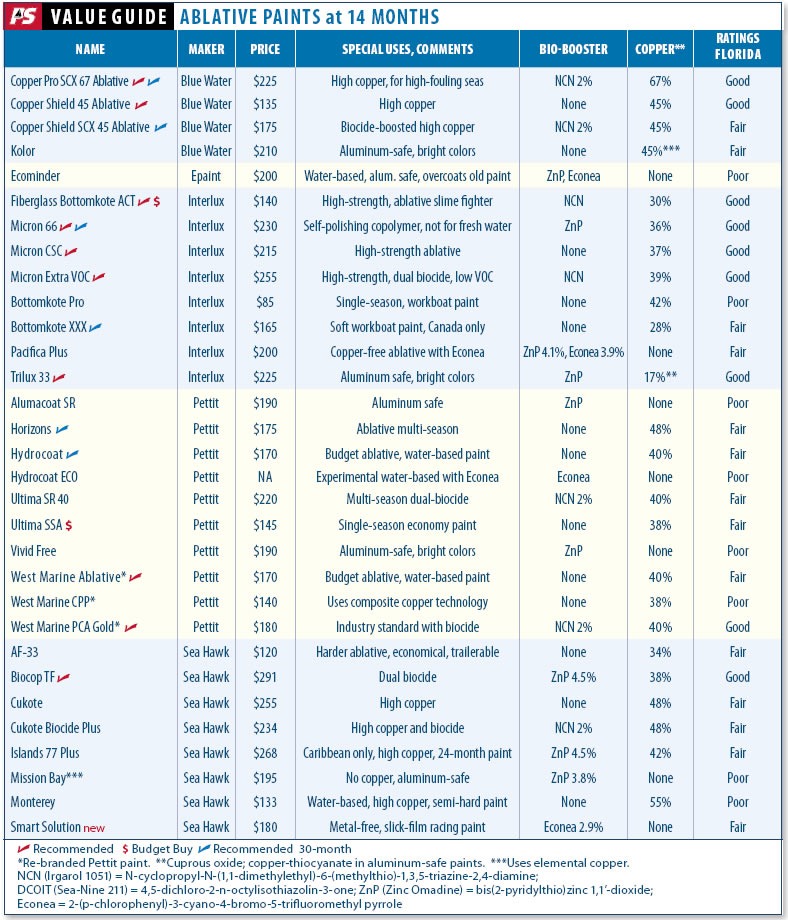
At 14 months, we begin to see two things: which paints keep your hull fast and smooth for a year, and which paints are likely to provide protection over the long term. Keep in mind that because we do not scrub or move our panels, you may see better performance over the short term. Because performance can vary with geography, we recommend consulting local experts, boatyards, and other boat owners to find what works in your area.
If you decide to clean the hull, take a conservative approach. Start with a sponge or T-shirt, and apply the least amount of pressure needed. If that doesn’t work, then move up to terry cloth. For even more muscle, move up to the green 3M scrub pad, a soft-bristle brush, or something similar. Once you need the scraper, it’s time to start planning a haulout.
Many ablative paints are designed to tolerate cleaning, but if you scrub hard at the outset, particularly on some softer ablative paints, you will literally be wiping your money away. Better to use the boat and let water action sluice the hull.
If you are using an ablative paint, you can also prolong the life of your protection by adding more than the recommended two coats. Some makers allow as many as four coats without risking adhesion problems. Check your manufacturer’s recommendations, and if you do use multiple coats, be sure to allow ample drying time.
Based on the performance of our 14-month panels, sailors looking for one to two years of protection against hard growth don’t need to pay a fortune. In the hard paints, Pettit’s Unepoxy and Blue Water Copper Shield 45 were Budget Buys. Pettit’s Unepoxy Plus and Copper Guard offer good value in the hard paint category. Blue Water’s Copper Shield 45 Hard is also a reliable low-budget contender. In the ablative category, there was a tie after 14 months, with Blue Water’s Copper Shield 45 Ablative ($135) and Interlux’s Bottomkote ACT ($140) offering the best value. Pettit Horizons and Sea Hawk AF-33 are also solid choices for the small-budget sailor.
A couple interesting Type 2 Volkswagen van ideas
Posted By RichC on February 24, 2012
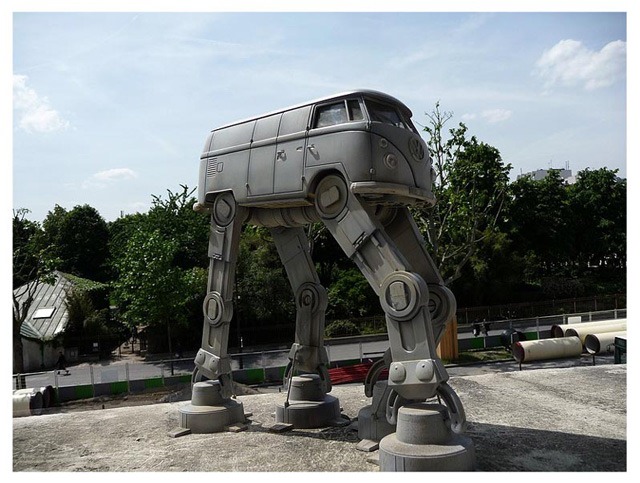 A Volkswagen diesel friend of mine and I tweeted a few messages back and forth yesterday after we noticed this interesting AT-AT Walker Microbus. He of course has a real VW van (1979) as well as a few ideas for a playhouse for his kids (below).
A Volkswagen diesel friend of mine and I tweeted a few messages back and forth yesterday after we noticed this interesting AT-AT Walker Microbus. He of course has a real VW van (1979) as well as a few ideas for a playhouse for his kids (below).

Even though I’m not really all that geeky (at least compared to others), I was impress with both the Starwars sculpture and the Volkswagen bus playhouse … I’d love to see one of these in his backyard (or maybe his “master bedroom” – obviously without his wife’s permission!)
Jeb Corliss still has something to learn from flying squirrels
Posted By RichC on February 23, 2012
Here’s a flying wingsuit jump that didn’t go as planned; the January 120mph collision with a mountain cliff isn’t something many adrenalin junkies survive to talk about. (broken legs and a 5 weeks in the hospital)
With tax uncertainty, how do we plan for retirement?
Posted By RichC on February 22, 2012
The tax season is upon us and many take this opportunity to take account of our retirement strategy (at least those who are thinking ahead). Years ago … in the days of the company pension, confidence in Social Security and Medicare and the assumption that one would retire at 65 after a lifetime career with a single company not has much thought was required … but times have changed. The pension is gone, the Social Security and Medicare system stressed and a guaranteed mid-60s retirement a thing of the past. On a positive note, some of us are healthier and will live longer and a few white collar employees or entrepreneurs may be fortunate enough to be healthy enough to work longer. What has changed nowadays is that we need to be accountable for our own retirement planning and that’s a challenge.
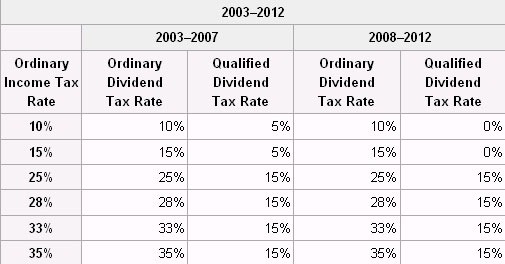
Current tax rates for those saving and planning for retirement around dividends
Not only are we faced with being responsible regarding the early saving for retirement in safe but growing investments that stay ahead of inflation, but also we need to navigate a challenging and changing tax code. From IRAs, Roth IRAs, 401Ks, Mutual Funds, ETF, corporate, government and treasury bonds, bank savings vehicles, 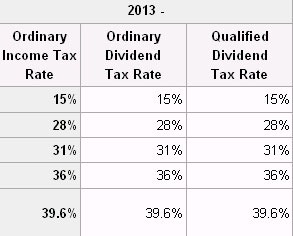 insurance products, stocks, real estate and trusts, we have complicated the process …which for many is like navigating a mine field; who has the tools or training to detect all of the hidden dangers? Add the federal governments tax code and future changes … and planning becomes a guessing game.
insurance products, stocks, real estate and trusts, we have complicated the process …which for many is like navigating a mine field; who has the tools or training to detect all of the hidden dangers? Add the federal governments tax code and future changes … and planning becomes a guessing game.
The recent hot potato item of taxing dividends is on the table for those currently retired or planning for it (possible increases for 2013 to the left). Now besides the “double taxation” associated with taxing a company’s income then re-taxing the distribution dividend to “owners,” the second tax also disproportionally impacts the savings and income seniors need to plan for retirement. If dividends are taxed at higher rates, this could discourage companies and their investors from long term investing … not to mention the income seniors are using to pay their cost of living expenses.
I understand that the government’s new goal is to tax the wealthiest Americans overall income (passive or earned) at higher rates and in turn increase the overall taxes they pay, but the targeting of twice taxed dividends at a time fewer and fewer retirees have other ways to save is a bad approach. I don’t love the Alternative Minimum Tax (AMT), but it make far more sense than raising taxes on dividends (personally I’d rather see a lower, but simplified tax – Steve Forbes tax postcard has always looked attractive to me).

Financial markets flirt with the psychological 13,000 mark
Posted By RichC on February 21, 2012
I watched the Dow break the 13000 mark a couple of times today, but unfortunately for bulls, it didn’t hold; the Dow closed up just .13% at 12966.  Looking back a few years, the Dow last traded at the 13000 level in May 2008 and was heading down from its historic high of 14198 in October 2007. I’m not sure we’re out of the woods just yet?
Looking back a few years, the Dow last traded at the 13000 level in May 2008 and was heading down from its historic high of 14198 in October 2007. I’m not sure we’re out of the woods just yet?
The real question is whether the financial markets will continue their rise even as tension with Iran push oil higher. Today oil closed over $106/barrel as most speculators are listening to the sabers rattle. This above $100/barrel oil has consumers funneling their dollars into their fuel tanks rather than helping the economy. We’re already tenuous as for as a recovery goes … higher transportation and shipping isn’t going to help. I can’t imagine what a new war or Israeli bombing of Iran would do?
When college age kids socially get the approval of parents
Posted By RichC on February 20, 2012
As I’ve mentioned before, one of the primary reasons I don’t post or visit my Facebook account very often is because it is the domain of my  kids and their friends. I’m sure I would not have wanted a nosy parent watching everything I said and did … so I didn’t focus on it as a parent; I gave them both privacy.
kids and their friends. I’m sure I would not have wanted a nosy parent watching everything I said and did … so I didn’t focus on it as a parent; I gave them both privacy.
That said, there are things I know have been posted that I don’t approve of … just as I’m sure there would have been in my day if social networking existed. BUT … today I noticed something positive (my opinion), as Taylor has both the masthead (sailing with Taylor last spring on Encore) and the Gipper as an avatar. It sure is nice to be able to nod in approval … and to secretly even pat myself on the back!
Desultory - des-uhl-tawr-ee, -tohr-ee
- lacking in consistency, constancy, or visible order, disconnected; fitful: desultory conversation.
- digressing from or unconnected with the main subject; random: a desultory remark.